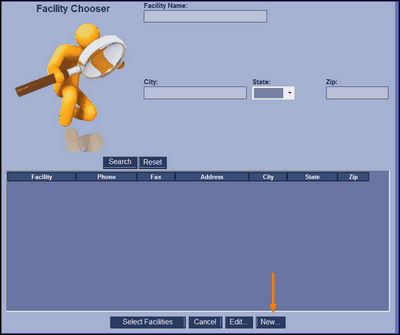
To create a new facility, click [New] to begin.
This is new facility screen. Enter all the information to create the new facility.
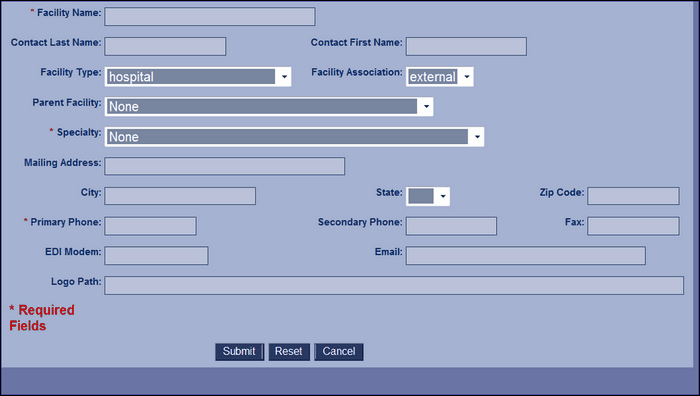
Facility Name |
The name of the new facility. This is a required field. |
Contact Last Name |
The last name of the contact person at the new facility. |
Contact First Name |
The first name of the contact person at the new facility. |
Facility Type |
The type of facility. The drop down box for this field includes several choices including hospital, medical equipment company, pharmacy, etc. |
Facility Association |
The association can be internal or external. Internal is the main building of a practice that may have many facilities. External is any facility that is associated with the practice but is not the main building of the practice. |
Parent Facility |
If the new facility is has an external association, the parent facility should be included. The drop down box contains a list of all existing facilities in HPN Chart. |
Specialty |
If a medical office, please include the specialty of the office. The drop down list contains a list of all the specialties listed in HPN Chart. New specialties can be added in the Manage Specialty List. |
Mailing Address |
The mailing address of the new facility. |
City |
The city of the new facility. |
State |
The state of the new facility. |
Zip Code |
The zip code of the new facility. |
Primary Phone |
The primary phone number of the new facility. |
Secondary Phone |
|
Fax |
|
EDI Modem |
|
Logo Path |